
How to Maximize Reimbursements for Rural Health Clinics
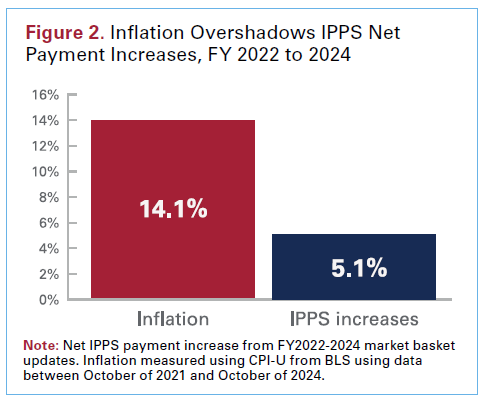
In 2023, hospitals absorbed $130 billion in Medicare and Medicaid underpayments — a roughly 14% annual increase over 2019.1 And underpayments are one reason providers can benefit from knowing how to maximize reimbursements for rural health clinics (RHCs). Why? Because a higher portion of RHC payments come from public sources compared to urban facilities, which makes addressing underpayments even more critical.
Medicare payment updates, like the finalized FY 2026 Inpatient Prospective Payment System (IPPS) 2.6% rate increase, will help.2 But, by themselves won’t be enough.
To protect your financial performance, you need consistent, proactive strategies to maximize reimbursements for your RHC’s revenue cycle.
The following best practices offer steps your RHC can take to better ensure reimbursements and improve your financial stability.
RHC Medicare Bundling Rules
Bundling rules are established Medicare policy. They define the services included in the All-Inclusive Rate (AIR) payment and that bill separately or are nonbillable under Medicare RHC guidelines. Understanding bundling rules that impact rural health clinic billing practices lets you ensure maximum and efficient reimbursements.
Some bundling rules differ for different types of RHCs, including independent and provider-based RHCs (PB-RHCs). For both independent RHC and PB-RHCs, the following bundling rules apply.
- Evaluation and management E/M visits are subject to (AIR) for qualifying visits
- Mental health services are subject to the AIR if core service is rendered
- Telehealth visits are subject to AIR with RHC specific HCPCS codes
- Minor procedures during a visit, such as wound care, or lesion removal, are bundled as part of a qualifying visit, such as a primary visit at the same time
- Injections or immunizations administered during visit when a vaccine is administered is bundled; the vaccine itself is billed separately
- Lab specimen collection (for example CPT 36415), is bundled into the AIR and not separately reimbursed
- Preventive services are paid at 100% of AIR and may be bundled with another visit on same date of service (DOS)
- Chronic care management (CCM) services aren’t bundled and are billed outside of a standard visit
- Transitional Care Management (TCM) aren’t bundled and are billed outside of a standard visit
- Remote Patient Monitoring (RPM) aren’t bundled and are billed outside of a standard patient care visit (CPT 99453 and 99454)
Billing categories that differ for RHC and PB-RHCs.
| Independent RHCs | PB-RHCs |
| Radiology (x-rays, ultrasounds) | |
| Not bundled; split billing to Medicare Part B< | May require split billing under parent hospital to Medicare Part A |
| Laboratory tests (CBC, urinalysis)< | |
| Not included in AIR, billed separately to Medicare Part B | Not included in AIR, billed separately under parent hospital |
At a high level, if a visit is part of the face-to-face provider encounter with an RHC-qualified practitioner, it’s bundled. If it’s diagnostic (lab, X-ray), durable (DME), or performed independently of a provider encounter, it’s not bundled.
More Bundling Tips
- Two visits for the same condition on the same DOS are bundled and paid as one AIR
- Medical and mental health visits on the same DOS aren’t bundled and are paid separately at the AIR rate
- Sick and preventative visits on the same DOS are bundled unless certain conditions (separate medically necessary illness or injury) occur, which lets them be billed and paid separately at the AIR rate
RHC 30-Day Rule
To ensure reimbursements for Medicare patients, knowing the 30-day rule is key. It applies to encounter-based, not fee-for-service billing. It specifies that if a Medicare patient has multiple same visit types (medical or mental health) at a rural health clinic within 30 days for the same condition, only one encounter is billable.
The exception is if the visits are clearly separate and distinct, and you show that the diagnosis/illness is unique from the preventive service.
Also, you can roll related services in a 30-day window into a single encounter and bill unrelated preventive services (AWV, IPPE) separately.
Medicare Credentialing and Recredentialing
eeping Medicare credentialing current is key to maximize reimbursements for rural health clinics. Delays or errors can cause denials, payment interruptions, or even termination.
You want to maintain a centralized log or checklist with an automated tracking system to track your renewal dates. Tracking with simple spreadsheets and calendar reminders can help prevent costly gaps as can credentialing software.
You also want to monitor the Provider Enrollment, Chain, and Ownership System (PECOS) regularly for accuracy and notifications and quickly make updates and/or respond to revalidation notices.
![]()
Want more like this? Sign up for emails and never miss an update! →
Common Denials That Affect Reimbursements
A great way to maximize reimbursements is to understand common denials and address them before they happen.
Eligibility and Insurance Coverage
Medicare coverage that shows as inactive or covered by another entity, such as Medicare Advantage, frequently causes denials for RHCs that treat large volumes of Medicare patients. Medicaid patients often have lapses or transitions between Managed Medicaid plans, and lapses in or loss of coverage may increase as a result of the One Big Beautiful Bill Act (OBBBA).
To reduce denials, run eligibility checks at scheduling and check-in, and use real-time automated verification and discovery tools to flag issues early.
Coding and Modifier Errors
Incorrect CPT/HCPCS, missing required modifiers (such as CG), or mismatched diagnosis/procedure commonly lead to denials.
To prevent issues, stay current on ICD-10 and CPT/HCPCS code updates, build and maintain claim edits or scrubbing tools in your electronic health record/practice management (EHR/PM) system, and ensure your staff are trained to spot and correct coding errors. Also consider automated tools to detect and flag missing codes for billers.
Bundling Errors
Claiming services separately that are already included in the RHC AIR, such as lab draws or minor procedures, can cause denials or recoupments.
To prevent issues, have the Medicare qualifying visit list accessible, keep a list of bundled versus unbundled service by type and a list of bundling rules for Medicare versus Medicaid, and configure your EHR/PM system to bundle correctly.
Prior Authorizations
Medicare Advantage and other payers will issue claim denials for services that require a prior authorization (PA) that wasn’t attained. And in 2026, traditional Medicare will require PA for certain services in six pilot states as part of the new CMS Wasteful and Inappropriate Service Reduction (WISeR) model.
To prevent denials now and as the WISeR model takes effect, maintain a list of services that require a PA broken down by insurance plan, document PAs with dates and reference numbers in the patient record, and build claim edits and alerts to flag claims with missing PA numbers before submission.
Also consider an AI-powered clinical billing assistant that can flag errors in real time, improve accuracy, and save your staff hours of manual work.
Strengthen Your Financial Health
By focusing on best practices, your RHC can help reduce financial risk, capture more accurate payments, and strengthen its ability to serve your patients for the long term.
Sources
1 American Hospital Association, The Cost of Caring: Challenges Facing America’s Hospitals in 2025, Apr. 2025, https://www.aha.org/sites/default/files/inline-images/Figure-2-Inflation-Overshadows-IPPS-Net-Payment-Increases-FY-2022-to-2024.png
{kind=link}
2 American Hospital Association, CMS Issues Hospital IPPS Final Rule for FY 2026, Jul. 31, 2025, https://www.aha.org/news/headline/2025-07-31-cms-issues-hospital-ipps-final-rule-fy-2026